







December 10 2020 - 12:39pm
Why has Pacific Asia “performed” so well on Covid-19? No country in this region has had an epidemic anything like as damaging as those in Europe, North America or South America — from Japan to South Korea, Australia to Taiwan.
The answer is of more than just epidemiological interest. Respect for the response of governments in this region has become a matter of political folklore — people like Jeremy Hunt talk about it all the time — and is fundamentally changing the reputation of the “Asian model” among the liberal commentariat. Where before there was scepticism and a distrust of the activist, technology-enabled, centralised control state, it is now commonly seen as having been more effective than Western democracies.
But some scientists think there are other factors at play, and that alongside the much-talked about cultural differences, border control, superior test and trace systems and the like there are biological reasons that explain why Asia has so far fared so well. If they are right, the implications are huge and would put an end to the idea that countries like the UK could ever have had outcomes like Taiwan or South Korea (which despite its recent surge in cases is still doing much better than Europe).
Of all the Asian countries, Japan is perhaps the most mysterious — a Northern hemisphere island nation full of old and theoretically vulnerable people which has largely eschewed lockdowns and yet, even as it enters its winter surge, is seeing numbers that any European country would envy. A September study of workers at a Tokyo company suggested that the proportion of asymptomatic people showing Covid-19 antibodies had gone from 5.8% to 46.8% over the summer, and that “infection may have spread widely across the general population of Tokyo despite the very low fatality rate.”
There have recently been a spate of new studies offering explanations for the “Asian exception”, and yet none has fully provided the answer.
The first is that there is something in the genes of East Asian people that make them more resistant to this particular virus. Researchers from Australia and the US found evidence of ancient genetic adaptation specific to East Asian populations that may have come from similar pandemics between 5,000 and 25,000 years ago. “An arms race with an ancient corona-like virus may have taken place in ancestral East Asian populations,” they concluded.
To support this idea, the Centre for Disease Control in the US estimates that whereas Covid-19 infection rates are between 1.4 and 1.7 times higher in African American, Native American and Hispanic populations than the white population, the rate for the Asian American population was 0.6 times the white average. But this theory still seems far-fetched to explain such dramatic differences, and of course doesn’t explain the differences in predominantly white countries like Australia and New Zealand — as one of the study’s co-author’s, David Enard of the University of Arizona, concluded, “if there is a genetic effect, it will be small to the point of being irrelevant.”
If it’s not a genetic difference, perhaps it is a difference of resistance or immunity? Given that SARS-Cov-1 originated in the region, there could have been other related coronaviruses circulating in recent years that provided cross-immunity. Recent evidence from the University of Boston suggests that recent infection with a related common cold coronavirus could dramatically reduce the severity of a Covid-19 infection. But so far there is a lack of evidence for this idea. Just yesterday, a group of scientists including Francois Balloux published a preprint detailing their search for a virus that might have increased T-Cell immunity, but so far they have found none. As Mark Lipsitch, Professor of Epidemiology at Harvard, put it to me, “it’s an interesting hypothesis. There’s no reason to believe it yet, but there’s no reason to dismiss it either.”
The alternative is that the difference is not caused by the people, but by the virus. The New York Times ran a story last week about a particular genetic strain of Covid-19 called D14G, that was demonstrably much more prevalent in Italy in the early months of the pandemic than any Asian countries and may have helped explain why the disease took off so dramatically in that country, and from there spread around Europe and America.
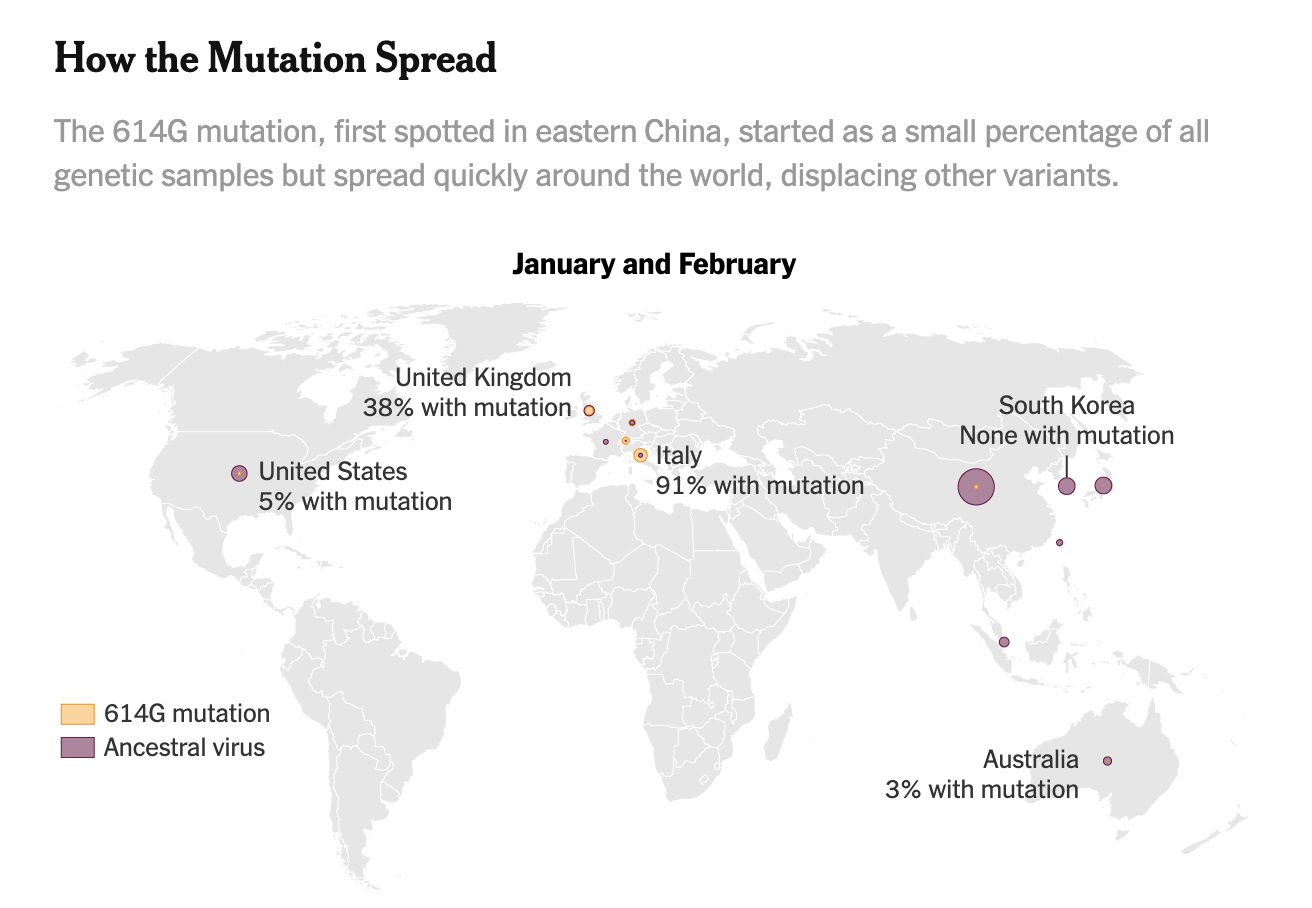
Today’s interview with David Engelthaler, co-director of the T-Gen Research Institute in Phoenix, Arizona, investigates this idea. His view is that there is now “more than a suggestion, leading to really compelling evidence” that this strain replicates faster than earlier strains. It doesn’t mean the mutation is more deadly, simply that it might be more effective at transmitting, which could help explain why the virus took off so dramatically in Europe and subsequently North America. He observed that several of the early introductions to Arizona, coming from the Pacific coast straight from China, fizzled out quickly, with less effective transmission. “And then all of a sudden we started having explosive outbreaks. When we go back and look genomically, the vast majority of those cases where we had very large outbreaks were being driven by the strains that were coming from the East Coast out of Europe, which all seemed to have this particular mutation in the spike protein.”
I put to Dr Engelthaler the obvious objection that the D14G strain of the virus is now dominant and has travelled back to Asia and across the world, but their rates remain much lower. Doesn’t that remove the variable? He accepted that it might not have been the driving effect, but pointed out: “you can’t compare the original introductions of this virus in one location to a reintroduction of a virus that’s already been going through a pandemic, where you have some amount of immunity built up and a lot of practices already in place.” In other words, the fact of different strains being around different parts of the world at crucial points in the cycle of the pandemic could have had a lasting effect on how well-seeded they became in those regions.
While this theory has been challenged by other research, it is certainly an interesting contribution to the debate. Better evidence may yet emerge for one or other of these explanations for the “Asian exception” —and of course the cultural habits and public policy responses will have played their part. But for now it seems wise to be sceptical of definitive statements about “what we could have done” with reference to Asian countries as proof. Like so much about the behaviour of this virus, notwithstanding the attempts by many commentators to pretend that we have all the answers, precisely why Asia has had such a different experience remains to be seen.
Freddie Sayers is the Editor-in-Chief of UnHerd and CEO of OQS Media. He was previously Editor-in-Chief of YouGov, and founder of PoliticsHome.
 freddiesayers
freddiesayers