







December 8 2021 - 7:00am
Johannesburg is known locally as the City of Gold, but this may not prove to be the case for vaccine manufacturers carefully watching the rapid spread of Omicron through Gauteng province. While compelling evidence has emerged that Covid’s latest variant is highly transmissible, the picture from local hospitals and testing data is that this wave may well pass quickly, without a large number of deaths and with an extremely high percentage of asymptomatic cases.
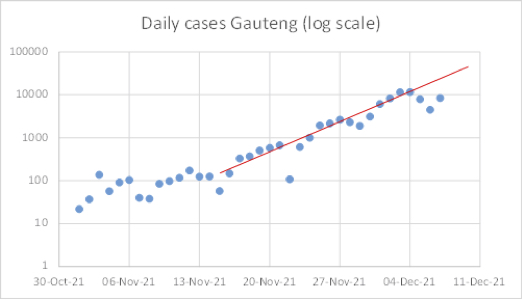
The local reproductive ratio is so high that the peak of cases may very likely occur in the next week (Tschwane is the city to watch) — far earlier than forecast. Indeed, yesterday’s total of 8,445 new cases in Gauteng was significantly lower than the logarithm regressions would have suggested and hints that a “pop and drop” pattern may already have started.
Using an another method of comparison, the previous Delta wave in Gauteng province took 59 days from start to peak (5th May to 3rd July 21). If we assume that Omicron spreads 2x faster than Delta, that would imply a 16th December peak; if it’s 2.5 x faster it would take us to 12th December; 3 x faster takes us to… yesterday. Test positivity (an important indicator given the limited testing capacity) has also plateaued.
Some will argue that this pattern will not replicate in the developed world. South Africa has a markedly younger population (although 20% suffer from HIV or AIDS) and has already endured three sizeable waves of Covid meaning that 60-70% of the population has developed some form of natural immunity along with the 30% who are fully vaccinated.
So far it is too early to tell how prior Covid and vaccination (albeit with waning as there is no local booster programme) will compare in terms of outcome. But the signs, based on the reports from local hospitals, are that both groups are susceptible to Omicron, albeit in a mild fashion when compared to Delta. The key question here is whether this is due to the ex-ante severity of Omicron itself, or to the infections and vaccines that have occurred since the summer months.
Of course, the current case data is far from adequate on its own. Tests are expensive in SA and largely occur in medical venues. Furthermore, community testing is very low in comparison to Europe. In addition, given more than half the cases (perhaps as many as 75%) are asymptomatic based on testing in the workplace, individuals are not rushing to test. This problem will repeat elsewhere and means that we may never see the dramatic peak in case numbers the modellers desire, but rather a petering out in the coming days in Gauteng — and a repeat in other parts of the globe.
Thus far, Western policy makers and advisors have pointedly chosen to describe local feedback from hospitals and GPs as “anecdotal,” falling back on the old refrain, “wait and see.” This patronising attitude reached new heights when the new German health minister said that he “prefers to wait for reports from the UK and Israel as data from Africa can be unreliable”. And while experts working from home are embraced daily in UK media, very little coverage has come from practitioners on the ground.
Rather than waiting for speculative results from vaccine companies (which will be unable to assess the impact on severe hospitalisation and death), experts must engage with the data we do have from Gauteng. Three of the most important observations to date relate to hospital duration (2.5 days with Omicron compared to 8.6 days with Delta), ICU occupancy (more than 60% lower) and oxygen usage (almost 70% lower). Given hospital data lags case data, monitoring how these figures evolve in the next two weeks will be key.
Moreover, in Europe there are already over a thousand tracked Omicron cases (largely double vaccinated and many are boosted); we need to hear if these individuals are asymptomatic or have mild symptoms and how they develop. Early evidence suggests that Omicron presents symptoms more quickly than Delta (2-3 days) so the peaks around the world may well be swift but short.
Finally, the singular focus on vaccination to the exclusion of everything else is unhelpful — given that Omicron is already spreading quickly through Europe, we need to accept that vaccines will not stop the spread of this variant nor future variants; their vital role is primarily to reduce severe cases and fatalities. Alongside this, prior Covid needs to be recognised as providing strong protection, and potentially longer lasting resilience given its mucosal advantage. Early results from a study examining effectiveness of vaccines against Omicron underline the importance of this phenomenon.
The doom and gloom narrative of politicians and financial markets is hopelessly out of sync with reality. It is clear that the world needs to open up again for travel. We need to introduce rapid testing wherever possible (rather than vaccine passports), and the politicians need to remember that the role of vaccines is not to provide a political tool to separate citizens on dubious statistical grounds which assume that waning does not exist.
We already know from Israel that the mRNA boosters are behaving in the same way as the second shots (i.e. waning notably in terms of transmission over 3-4 months) and hence point estimates of vaccine efficacy on transmission are of little use. Recent focus on vaccines for children (where the odds of severe Covid are incredibly low), restrictions on the unvaccinated, calls for renewed lockdowns and insatiable demand for updated booster shots, only highlight just how far away from evidence-based Science we have drifted.
Anthony Clake is a partner at Marshall Wace LLP and writes in a personal capacity.
Join the discussion
Join like minded readers that support our journalism by becoming a paid subscriber
To join the discussion in the comments, become a paid subscriber.
Join like minded readers that support our journalism, read unlimited articles and enjoy other subscriber-only benefits.
Subscribe