







September 7 2022 - 4:08pm
Science does not operate independently from the realms of politics and culture. This was no more evident than with the coronavirus pandemic: questions of epidemiological modelling, the efficacy of lockdowns, vaccine mandates and social distancing all saw the world split into different camps. And whatever position one took on lockdowns, for example, became convenient shorthand for their politics writ-large.
The emerging question of continuing excess deaths in the aftermath of Covid has not escaped this phenomenon. It may turn out to be as polarising as any other Covid-19 controversy. Over the past three months the number of excess deaths in the United Kingdom – that is the amount of people actually dying compared to the amount of people expected to die – has been consistently trending upwards. And over the past ten weeks deaths have been in excess by 15%.
The contours of the debate are becoming clear. On one hand, there are those insistent that the deaths are linked, in some way, to the Covid vaccines. On the other hand, establishment voices reject that theory wholesale, and instead suggest the excess is tied to the lasting impacts of Covid infections, illnesses that went undiagnosed thanks to lockdown, and a myriad of other complicating factors.
Stuart McDonald, head of Demographic Assumptions and Methodology at Lloyds Banking Group, sees this split as an unfortunate by-product of the pandemic more generally: people are jumping to assumptions to satisfy their preconceived ideas about the world before fully interrogating the data. What we know for certain is that more people are dying than we would expect: “It’s an undeniable fact.”
Working out why is a much harder task. On inspection of the data, however, it is clear that some of these deaths are disproportionately attached to certain health conditions: “The majority of the cases are cardiovascular, circulatory, cerebrovascular.”
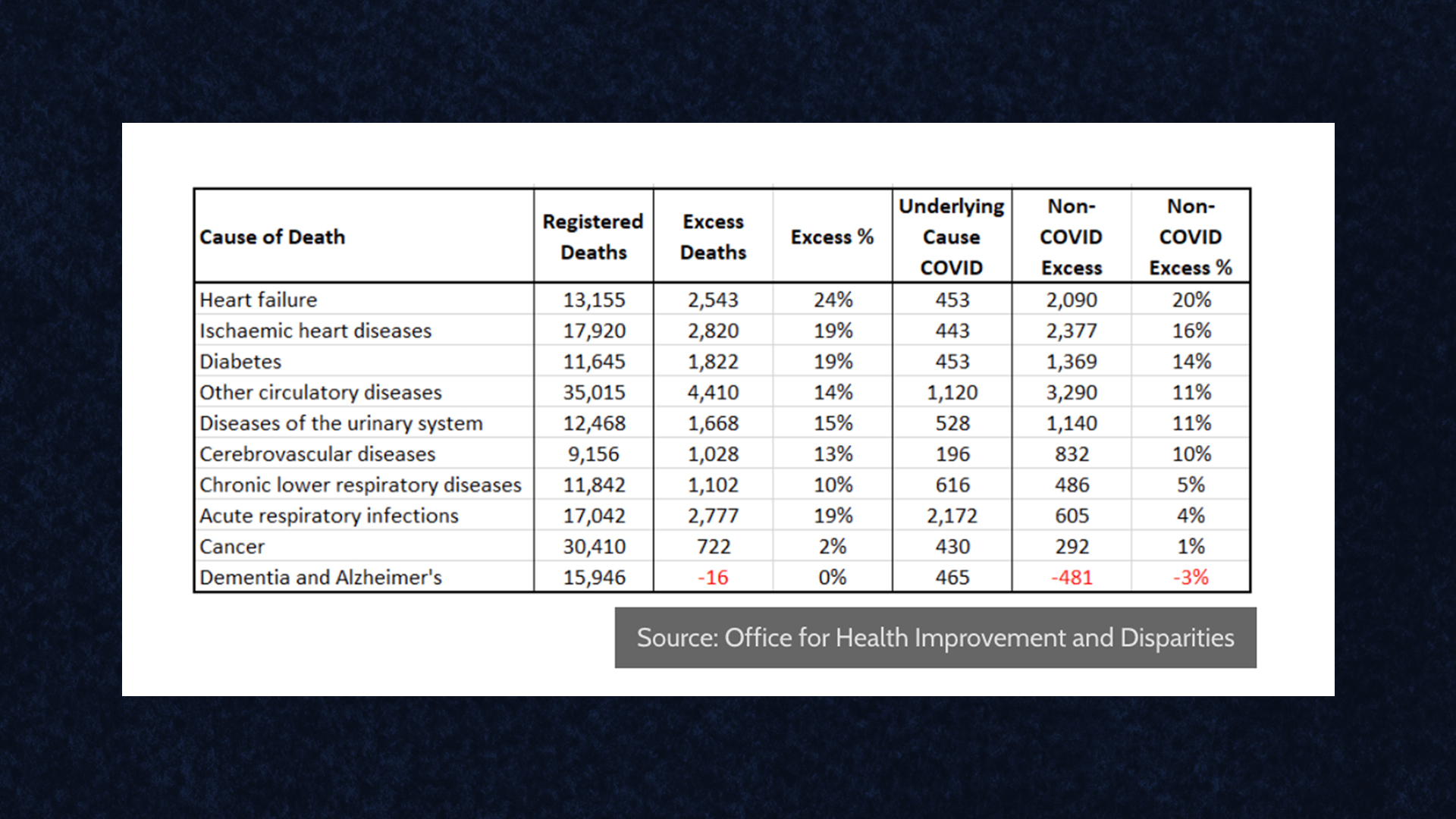
But death certificates, McDonald explains, often list several causes. And those causes can be hard to disentangle from one another. The above table shows there are 13,155 deaths in some way linked to heart failure, and “only a very small proportion of those had Covid as the underlying cause.” But, “if we look at the chronic lower respiratory diseases, or the acute respiratory infections, the majority of excess deaths we’re seeing in those two cases may actually be attributable to Covid.”
Those wary of the longer-term side effects of the vaccine may take energy from this table. If we have a strong indication that cardiovascular deaths are particularly elevated, and we know that officially accepted side effects of the mRNA vaccines are myocarditis and pericarditis, might these things be connected?
McDonald is unconvinced. Post-viral cardiovascular issues are well-known and well studied consequences of other viruses. “We have historic evidence of elevated cardiovascular risks extending beyond the immediate acute infection, and we have pretty firm evidence that there are a sub-group of people who have had Covid-19 that will experience elevated cardiovascular risks” he explains.
Overall, to further challenge the arguments of the vaccine sceptics, “the data consistently shows that the fully vaccinated have a lower mortality rate than those that are unvaccinated.”
“The vaccine could simultaneously be reducing the risk of the vast majority and also be putting a small number – a very small number – at elevated risk. This is why vaccine trials take place. And this is why the vaccine has been very carefully monitored since its rollout. And indeed, there have been changes to recommendations made about which vaccines we give to certain age groups based on the reports of those rare side effects.”
We cannot 100% rule out any impact of the vaccine on these excess death figures. But “there are so many stronger hypotheses than that one,” McDonald argues.
Among these is the acute pressure currently suffocating the NHS. The target ambulance response time, for example, is 18 minutes. In July the average wait time is 59 minutes. When it comes to strokes and heart attacks, fast action is the most effective treatment. And so, “if it takes nearly an hour to get an ambulance to these people, then sadly, there will be more deaths.”
It is not just the current state of ambulance response times, however. The lockdown itself caused significant behavioural changes in people who would otherwise have sought medical attention.
“While lockdowns didn’t prevent people from seeking care legally, there was a behaviour change. People were not accessing treatment at hospitals to avoid a perceived risk of contracting Covid. And that’s had knock on effects: with elective non urgent care waiting lists have grown, up more than 50% since before the pandemic. Now around 6.7 million people are on those lists.”
This is playing out in the statistics as well. “We expect a certain number of people to come forward with medical concerns every year – lumps, other things that usually cause worry. Those numbers fell, and they fell substantially, particularly during the first lockdown.”
One of the biggest concerns during lockdown – particularly among those more sceptical of the project – was that it would cause delayed cancer diagnoses, and ultimately a big spike in cancer deaths. That is not currently observable in the data. But McDonald is keen to stress that the fears about cancer deaths were legitimate.
Both the disruption the health service experienced as a direct impact of Covid, and also the actions we took to mitigate the spread of Covid, affected the number of cancer diagnoses doctors were able to make. “This will mean a worse prognosis and shorter life expectancies for cancer patients who ought to have been diagnosed a year or two ago” McDonald argues. But that is likely to play out over a much longer time period. Cancer delays are not playing a material part in the current excess, but it is uncontroversial to suggest that they will come.
A consensus has yet to emerge on the causes behind the UK’s troubling death figures. And this makes the whole topic fertile ground for the culture warriors. It seems clear that hospital delays are a significant – if not the most – significant factor. But we are still in the early days of analysing this phenomenon, and far from any kind of certainty.